In the context of PALS, suctioning plays a crucial role in airway management, particularly during cardiac arrest and other emergency situations.
Here’s an overview of suctioning in PALS:
Purpose of Suctioning in PALS:
1. Clearing Airway Obstruction:
– Suctioning is employed to remove secretions, blood, vomitus, or other foreign materials that may obstruct the patient’s airway.
– Airway patency is essential for effective ventilation and oxygenation during resuscitation efforts.
2. Facilitating Ventilation:
– In scenarios where a patient’s airway is compromised by fluids or debris, suctioning helps ensure unobstructed airflow for ventilation.
– Effective ventilation is critical in maintaining oxygenation and preventing hypoxia.
3. Enhancing Visualization:
– During advanced airway procedures such as endotracheal intubation, suctioning assists in clearing the airway for better visualization of the vocal cords and tube placement.
Procedure for Suctioning in PALS:
Assessment:
– Evaluate the need for suctioning based on clinical signs such as gurgling sounds, visible secretions, or airway obstruction.
Prepare Equipment:
– Ensure the suction unit is functional and properly connected.
– Choose an appropriate suction catheter size for the patient.
Position the Patient:
– Position the patient appropriately to facilitate suctioning, considering the patient’s condition and any ongoing resuscitation efforts.
Preoxygenation:
– Administer high-flow oxygen to the patient before and after suctioning to optimize oxygen levels.
Suctioning Technique:
Suctioning is carried out utilizing either a flexible or rigid catheter connected to a suction unit, which can be wall-mounted or portable. The suction unit is equipped with a pressure gauge to indicate the negative pressure (suction force) and a collection canister.
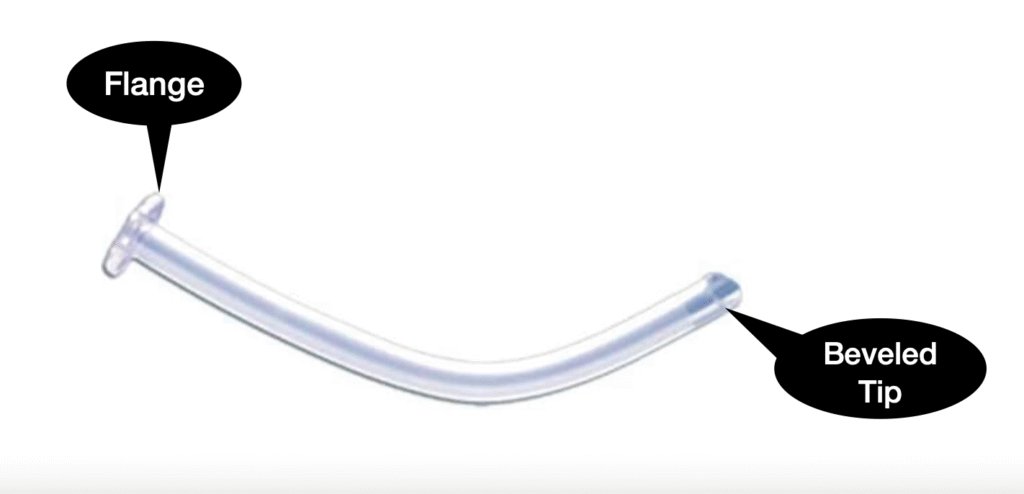
– Flexible Catheters:
– Suitable for eliminating thin, fluid secretions from the oropharynx or nasopharynx.
– Inserted through the mouth or nose.
– A sterile flexible catheter is employed for suctioning an endotracheal tube.
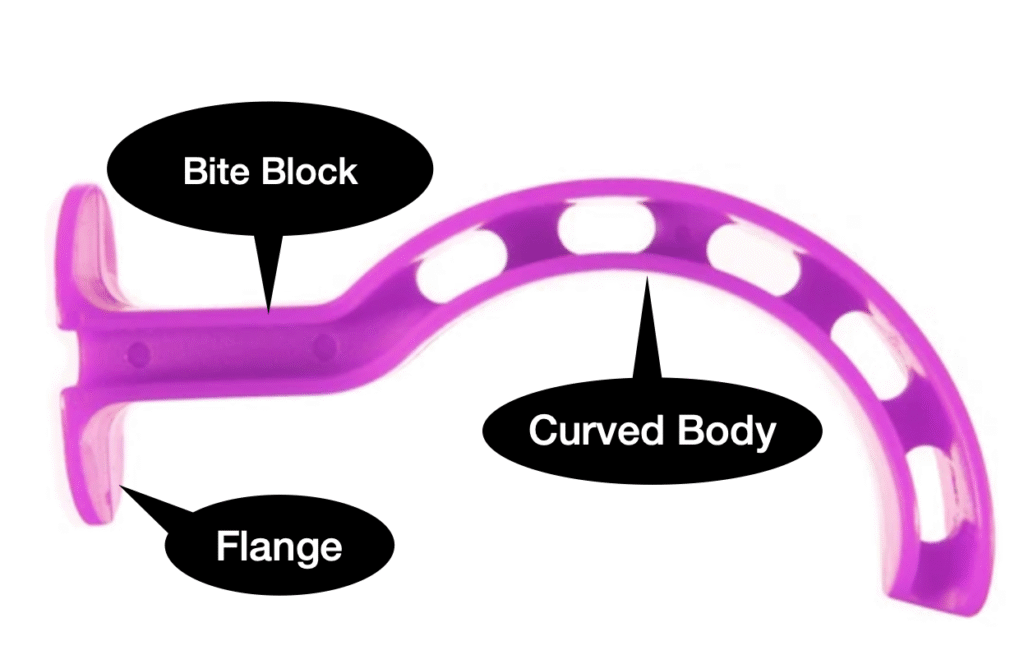
– Rigid (Yankauer) Catheters:
– Designed for removing thick or particulate matter from the oropharynx.
– Inserted through the mouth.
– Insert the suction catheter into the airway while applying intermittent suction during withdrawal.
– Limit each suctioning pass to 10 seconds to minimize the risk of hypoxia.
– Monitor the patient’s oxygen saturation and vital signs throughout the procedure.
Repeat as Needed:
– Repeat suctioning as necessary, reassessing the airway and patient response.
Post-Suctioning Care:
– Provide additional oxygen and reassess the effectiveness of ventilation.
– Address any ongoing airway management needs.
Considerations:
– Suctioning should be performed cautiously to prevent complications such as hypoxia or tissue trauma.
– Regular reassessment of the airway and the patient’s response is essential during suctioning in PALS.
Suctioning is a vital component of airway management in PALS, ensuring the maintenance of a clear and patent airway during resuscitation efforts. It is crucial for healthcare providers to be proficient in suctioning techniques and integrate them seamlessly into the overall care of the patient in emergency situations.
Waveform Capnography:
What is Waveform Capnography?
Waveform capnography measures the amount of carbon dioxide (CO2) in exhaled air, which provides information about the patient’s ventilatory status. It displays this information in both numerical form (end-tidal CO2, or EtCO2) and as a waveform, allowing for continuous monitoring.
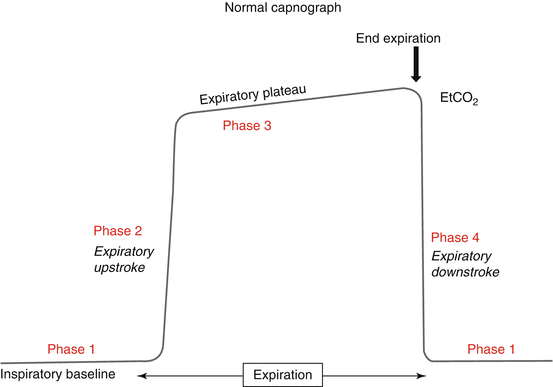
Components of the Capnography Waveform
The capnography waveform, also known as a capnogram, consists of several phases:
1. Phase I : Baseline, representing exhalation of CO2-free gas from the anatomical dead space.
2. Phase II: Expiratory upstroke, where CO2 from alveolar gas starts to mix with dead space gas.
3. Phase III: Alveolar plateau, where alveolar gas is exhaled and the CO2 level reaches a plateau.
4. Phase IV: Inspiratory downstroke, where fresh gas without CO2 is inhaled.